The answer to that question is apparently up to us.
I've been working on a research project dealing with health care opportunities - nothing at all to do with Obama Care - just a small piece of contract work that's part of a bigger economic development research project.
I want to share an interesting bit from my research. The reason I'm posting it is because the data I've reviewed suggests that we CAN control health care costs, and that the aging of our boomer population doesn't have to have either the frightening cost correlations the nation is anticipating, nor the even more fearful prospect - for boomers like me, anyway - that old people will have to go without treatment. Citations are all fairly to very recent, and mostly institutional - Deloitte, World Bank, WHO, etc. - or peer reviewed journal studies.
"Health care is a multi-trillion dollar expense world-wide. The World Health Organization [WHO] reports that 2011 world health care costs were at $6.5 trillion in U.S. dollars, with eighty-four percent of that amount spent on only 18 percent of the world’s population, in the wealthier 34 countries belonging to the Organization for Economic Cooperation and Development [OECD]. Spending across all WHO member nations averages $4380 per person, or approximately 12.4 percent of the national GDP, but those figures are misleading because the range among countries is quite extreme. Average per person spending on health care ranges from a high of $8,362 in the United States to $12 in Eritria. Countries in the African region spends about 6.5% GDP, South East Asian region spends 3.7 % GDP, or $83 U.S. dollars and $ 48 U.S. dollars respectively.3
Health spending is rising everywhere, but most notably at the wealthiest OECD countries where health spending exceeds GDP growth substantially. To understand the rate of growth, in 1960 health spending accounted for under four percent of GDP on average across OECD countries. By 2009, the average had risen to 9.6 percent, to a high of 12 percent in several countries. The United States, the outlier, spent over 17 of its GPD in 2009. Interestingly, looking at outcomes shows very little correlation between better outcomes and marginal increases in health care spending, suggesting that increased efficiencies are necessary to ensure maximum benefit from health care expenditures.12
It is anticipated that the cost of health care will continue
to rise. Although aging is often the
reason cited, it is important to note that aging per se is not the most
important factor in rising health care costs. The aging of the population by itself adds approximately half a percentage point to the annual growth in per capita health spending in industrialized societies.26 Instead, data shows that the most significant health spending occurs in the proximity to death, regardless of age of death. In fact, health care near death tend to be
higher for the young and middle aged than for elderly people.22 It is inevitable that there will be a growing number of elderly deaths in countries
with a aging population, due to costs associated with the pre-death
years. Yet the importance of drilling down into the actual cost sources - rather
than labeling the problem one of aging – makes the difference between a sense
of the inevitability of rising health care costs, as opposed to focusing health care
policy, practice and research on specifics that can reduce costs dramatically - predictably enough to offset the sheer numbers due to aging. If
the structuring and choice of medical treatment for patients near the end of
life can be controlled through preventative care, managed care, reduced expense
technologies, shifts in health service provider training, long-term shared funding
mechanisms, and other mechanisms, then aging per se does not need to have a
disproportionate bearing on health costs.24
By way of example, technological progress since 1998 has reduced the number
of overnight hospital admissions in favor of day admissions and clinic visits, and
reduced stay length. Technology has enabled
in-office detection and treatments of some diseases, such as diabetes, further reducing
hospital admissions and costs. The integration of care
programs, such as cardio-specific treatment units, has also impacted costs by
bringing specialists, best practice treatment protocols and equipment into one
location.25 Conversely,
costs associated with pharmaceutical uses have driven end of life costs up significantly
over time, and bringing drug prices down should be a future focus for research and innovation.24.
Identification of high cost drivers can focus
policy-makers, health care systems and researchers on areas high impact for both policy and practice change."
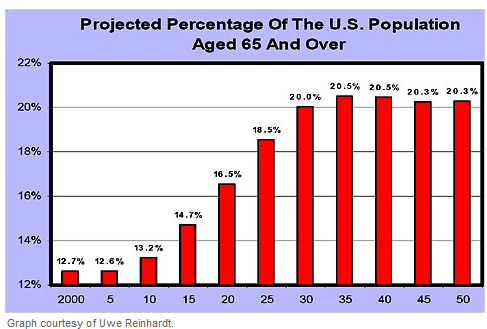
Here is another depiction of the first graph, just for fun. Look how much less frightening it looks if you don't put 22 percent at the top of the chart, but look at the growth of our aging population on a 100 percent scale.

By the way, here is another little tidbit from my research that might be interesting to share:
Here is another depiction of the first graph, just for fun. Look how much less frightening it looks if you don't put 22 percent at the top of the chart, but look at the growth of our aging population on a 100 percent scale.

By the way, here is another little tidbit from my research that might be interesting to share:
"All countries except Chile, Mexico and the United States finance health care primarily through the public sector. On average, over the past 20 years, the public share of health spending has remained at about 72 percent of total health care costs. However, this average is somewhat misleading, as health care reform attempts in some countries have impacted that percentage downward, while the expansion of public health insurance coverage has nudged it up elsewhere. Interestingly, spending more per capita is only nominally correlated with life expectancy, suggesting improvements are still needed to tie better health care outcomes more directly to additional moneys spent."12
I don't have time right now because it has nothing at all to do with my research project, but eventually, I'd like to take a look at the other two privately-funded health care systems, in Chile and Mexico, and see how it's working for them. Below is a chart demonstrating the gap between the U.S. and other industrialized countries.


3.
Etienne, C. (2012). World Health Expenditure
Atlas. Geneva: WHO, http://www.who.int/nha/atlas.pdf.
12.
www.oecd.org
22.
Oliveira Martins, J., & De la Maisonneuve,
C. (2006). The drivers of public expenditure on health and long-term care: an
integrated approach, http://www.agri-outlook.org/dataoecd/62/19/40507566.pdf
23. Gottret, P. E., & Schieber, G. (2006).
Chapter 1: Health transitions, disease burdens, and health expenditure patterns
Health financing revisited: a practitioner's guide (Vol. 434): World Bank
Publications, http://siteresources.worldbank.org/INTHSD/Resources/topics/Health-Financing/HFRChap1.pdf
24. Palangkaraya, A., & Yong, J. (2009).
Population ageing and its implications on aggregate health care demand:
empirical evidence from 22 OECD countries. International journal of health care
finance and economics, 9(4), 391-402.
25. De Meijer, C., Koopmanschap, M., Van Doorslaer,
E., & O'Donnell, O. (2012). Health Expenditure Growth: Looking beyond the
Average through Decomposition of the Full Distribution, http://repub.eur.nl/res/pub/32666/2012-0513%5D.pdf
26.
Reinhardt, U. E. (2003). Does the aging of the
population really drive the demand for health care? Health Affairs, 22(6),
27-39, http://142.36.155.4/cmt/39thparl/session-4/health/submissions/Reinhardt_Does_The_Aging_Of_The_Populations_Really_Drive_The_Demand_For_Health_Care_2003.pdf