A couple of new eco-conscious products I'm trying this month:
Clean Ones Pure Comfort reusable vinyl gloves are latex-free, BPA-free and phthalate-free. I'm not personally allergic to latex, a natural material from a rubber plant. But those who are can go into anaphlactic shock, so it seems like too big a risk to have them around.
Another product I'm trying this month is Seventh Generation's dish soap. I've avoided it until now because it's pricey, but I found a great deal on Amazon.com - six 25 oz bottles for $15.48. That's just over $2 a bottle. I'm probably going to give away five of the bottles and ask that people try the product and then buy a refill product to use in the bottle, because I object to the disposability. I think they should either concentrate this product or offer it in larger quantities so that we can refill one bottle. Shipping small bottles is transportation-excess and creates too much CO2. I did find a 36 oz refill, and although the packaging is lighter weight than the bottles, it's not different enough size-wise to make the transportation-reduction impact a larger-sized refill - or even better, a concentrate product - could make. If someone knows whether Seventh Generation has a concentrate in this product, please let me know. I didn't see one on their website.
The answer to that question is apparently up to us.
I've been working on a research project dealing with health care opportunities - nothing at all to do with Obama Care - just a small piece of contract work that's part of a bigger economic development research project.
I want to share an interesting bit from my research. The reason I'm posting it is because the data I've reviewed suggests that we CAN control health care costs, and that the aging of our boomer population doesn't have to have either the frightening cost correlations the nation is anticipating, nor the even more fearful prospect - for boomers like me, anyway - that old people will have to go without treatment. Citations are all fairly to very recent, and mostly institutional - Deloitte, World Bank, WHO, etc. - or peer reviewed journal studies.
"Health care is a multi-trillion dollar expense
world-wide. The World Health
Organization [WHO] reports that 2011 world health care costs were at $6.5
trillion in U.S. dollars, with eighty-four percent of that amount spent on only
18 percent of the world’s population, in the wealthier 34 countries belonging
to the Organization for Economic Cooperation and Development [OECD]. Spending across all WHO member nations averages
$4380 per person, or approximately 12.4 percent of the national GDP, but those
figures are misleading because the range among countries is quite extreme. Average per person spending on health care
ranges from a high of $8,362 in the United States to $12 in Eritria. Countries in the African region spends about
6.5% GDP, South East Asian region spends 3.7 % GDP, or $83 U.S. dollars and $
48 U.S. dollars respectively.3
Health spending is rising everywhere, but most notably at the wealthiest OECD countries where health spending exceeds GDP growth substantially. To understand the rate of growth, in 1960 health spending accounted for under four percent of GDP on average across OECD countries. By 2009, the average had risen to 9.6 percent, to a high of 12 percent in several countries. The United States, the outlier, spent over 17 of its GPD in 2009.Interestingly, looking at outcomes shows very little correlation between better outcomes and marginal increases in health care spending, suggesting that increased efficiencies are necessary to ensure maximum benefit from health care expenditures.12
It is anticipated that the cost of health care will continue
to rise. Although aging is often the
reason cited, it is important to note that aging per se is not the most
important factor in rising health care costs. The aging of the population by itself adds approximately half a percentage point to the annual growth in per capita health spending in industrialized societies.26 Instead, data shows that the most significant health spending occurs in the proximity to death, regardless of age of death. In fact, health care near death tend to be
higher for the young and middle aged than for elderly people.22 It is inevitable that there will be a growing number of elderly deaths in countries
with a aging population, due to costs associated with the pre-death
years. Yet the importance of drilling down into the actual cost sources - rather
than labeling the problem one of aging – makes the difference between a sense
of the inevitability of rising health care costs, as opposed to focusing health care
policy, practice and research on specifics that can reduce costs dramatically - predictably enough to offset the sheer numbers due to aging.If
the structuring and choice of medical treatment for patients near the end of
life can be controlled through preventative care, managed care, reduced expense
technologies, shifts in health service provider training, long-term shared funding
mechanisms, and other mechanisms, then aging per se does not need to have a
disproportionate bearing on health costs.24
By way of example, technological progress since 1998 has reduced the number
of overnight hospital admissions in favor of day admissions and clinic visits, and
reduced stay length. Technology has enabled
in-office detection and treatments of some diseases, such as diabetes, further reducing
hospital admissions and costs. The integration of care
programs, such as cardio-specific treatment units, has also impacted costs by
bringing specialists, best practice treatment protocols and equipment into one
location.25 Conversely,
costs associated with pharmaceutical uses have driven end of life costs up significantly
over time, and bringing drug prices down should be a future focus for research and innovation.24.
Identification of high cost drivers can focus
policy-makers, health care systems and researchers on areas high impact for both policy and practice change."
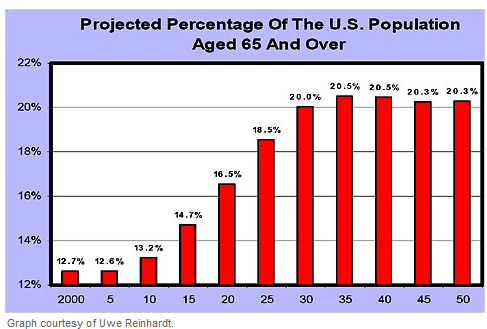
Here is another depiction of the first graph, just for fun. Look how much less frightening it looks if you don't put 22 percent at the top of the chart, but look at the growth of our aging population on a 100 percent scale.
By the way, here is another little tidbit from my research that might be interesting to share:
"All countries except Chile, Mexico and the United States finance health care primarily through the public sector. On average, over the past 20 years, the public share of health spending has remained at about 72 percent of total health care costs. However, this average is somewhat misleading, as health care reform attempts in some countries have impacted that percentage downward, while the expansion of public health insurance coverage has nudged it up elsewhere. Interestingly, spending more per capita is only nominally correlated with life expectancy, suggesting improvements are still needed to tie better health care outcomes more directly to additional moneys spent."12
I don't have time right now because it has nothing at all to do with my research project, but eventually, I'd like to take a look at the other two privately-funded health care systems, in Chile and Mexico, and see how it's working for them. Below is a chart demonstrating the gap between the U.S. and other industrialized countries.
3.Etienne, C. (2012). World Health Expenditure
Atlas. Geneva: WHO, http://www.who.int/nha/atlas.pdf.
24. Palangkaraya, A., & Yong, J. (2009).
Population ageing and its implications on aggregate health care demand:
empirical evidence from 22 OECD countries. International journal of health care
finance and economics, 9(4), 391-402.
25. De Meijer, C., Koopmanschap, M., Van Doorslaer,
E., & O'Donnell, O. (2012). Health Expenditure Growth: Looking beyond the
Average through Decomposition of the Full Distribution, http://repub.eur.nl/res/pub/32666/2012-0513%5D.pdf
26.
Reinhardt, U. E. (2003). Does the aging of the
population really drive the demand for health care? Health Affairs, 22(6),
27-39, http://142.36.155.4/cmt/39thparl/session-4/health/submissions/Reinhardt_Does_The_Aging_Of_The_Populations_Really_Drive_The_Demand_For_Health_Care_2003.pdf
How do you know whether your community is truly making progress on the march to Sustainable living?
You can get a whole lot better at answering that question with the right measuring tools. One of the resources I use with my sustainability classes is freely put out by an organization called "Whole Measures." Whole Measures is a "tool center" for Whole Communities developed to help communities describe and measure the relationships they want to foster between land and people. It employs a highly integrated, whole systems approach that looks at a variety of communal and environmental issues, including biodiversity, social equity, human rights, civic engagement, and landscape-scale conservation.
If your organization is looking for such tools, you might consider attending one of the Whole Measures Workshops. They are being held Tuesday, July 10 through Friday, July 13 at Center for Whole Communities, Knoll Farm, Vermont, and again Tuesday, December 4 through Thursday December 6 at Interaction Institute for Social Change in Boston, Massachusetts.
I am a person who rejects these four little words:
"It can't be done."
While I do occasionally spin my wheels trying to figure out how to cross a bridge that's just not there, for the most part, I have come to believe that human creativity, passion and good faith is a recipe for problem-solving.
So, when I think about solving the big, big problems facing our planet right now - whether it's the huge economic crisis, world hunger, the AIDS epidemic, climate change or whatever, I believe in outside-the-box thinking. I believe in turning a problem over and over and over until it no longer even looks like the original problem. Creative re-imagining. That makes it easier to solve.
What do I mean by that? Well, we all have ideas about how things can and will work - preconceived notions. These preconceived notions act as mental blocks. They get in our way of finding novel solutions. To get around our preconceived notions, we have to change the way we look at a problem, so that it doesn't look like the "same old problem," so that our same old beliefs about solving the problem do not trigger.
So, you ask, how does one "turn a problem over and over until it no longer looks like the original problem"? Have you ever said a word over and over so many times that it no longer held meaning for you? It's something like that. Only instead of stating the problem over and over again, you state the problem from a different angle.
Anthony Weston, a philosopher who's books I use when trying to teach outside-the-box thinking to my students and nonprofit clients, uses the example of a woman who will die if she does not get a particular medication, but the medication is so expensive that her family cannot afford it. The husband goes to the pharmacist and pleas for his wife's life. He offers everything he can scrape up, after selling all their worldly belongings, but it is not enough, and the pharmacy refuses to sell. The husband's dilemma: to steal the medicine or watch his wife die.
Most of my students immediately go to the preconceived choice set: an ethical discussion about whether stealing might be permissible in this case. Rather like the conversations we had about folks whose lives were washed away by Hurricane Katrina, and so took food from abandoned stores in order to feed their families. Which is the greater bad?
But Weston points out that we are not actually stuck with this "either/or" choice. When he's encouraged his students to think outside the box, they've come up with really novel solutions ranging from starting a nonprofit to make grants to people who cannot afford medication, to having the wife steal her own medication, and steal it as clumsily as possible, so that when she gets caught and goes to jail, she will receive the medical care she needs. Prisoners get medical care at the state's expense!
Another exercise that helps people get creativethink outside the box: how many uses can you come up with for a paperclip? When I group students and ask them to tackle that question, we get great lists. Groups might come up with 15 or even 50 ideas. But that's it. If I then ask them to rethink the paperclip, e.g. What if the paperclip is two feet tall? What if the paperclip could float? What if the paperclip could fly?What if the paperclip were made out of rubber? Suddenly their lists grow exponentially. It's simply a matter of removing their self-imposed limitations.
There are some great folks out there already thinking outside the box on some of our most difficult problems.
Take, for example, microfinancing. Somewhere along the way, some really creative folks got the idea that people could be helped out of poverty with very small loans - just enough to purchase something that they could resell for a profit, and then repeat the cycle until they had enough profit coming in that they no longer needed the loans to make their wholesale purchases. However, traditional lending institutions do not lend money to indigent borrowers. Traditional lending institutions have criteria for lending that significantly reduces risk, and so do not lend to folks who do not have either a lot of collateral or a history of repayment. Into this void stepped nonprofit organizations like Accion International and Grameen Bank and others who offer small loans and business training to the poor.
Another example of out-of-the-box thinking at work: I have become friends with the vintners at Peterson Winery, who produce a superb product, yet manage to keep their bottle prices lower than some of the other local wineries whose product is on par with theirs. One of the ways they do that is to "sell futures" in their wine. Faithful customers who trust the Petersons' wine making acumen are given the opportunity to buy Peterson wines in advance, at a discount. This is happy for everyone. The Petersons are, in effect, taking loans from their customers, free of interest, to cushion their operating costs until the wine is ready for purchase. The customers get a bargain, not to mention interest-free money helps the Petersons keep their wine prices down.
What started me on this little out-of-the-box diatribe this morning?
Well, two great out-of-the-box ideas that make a big difference, from FastCoExist.com, showed up in my email this morning.
The first idea is a cross between the microfinancing banks and the Petersons' customer pre-funded purchases. "Credibles" turns consumers into lenders, who in effect pre-fund their favorite slow food businesses, and then get their loans repaid in product. The difference between Credibles and Peterson Winery is that lenders may take repayment in product from any of the slow food businesses participating in the Credibles program.
The second is a really, really funny, very, very clever out-of-the-box solution, is a new idea for convincing Mexico's dog owners to pick up their dog's poo. The parks agency has installed poo containers that, when the contents reach a certain weight, turn on free wi fi for the entire park. This encourages not only dog owners, but others who want wi fi, to don a plastic glove and clean up the park! Now I call that truly creative thinking.
No need to limit all this creativity to fixing the world, however. If you think you might want to get better at creatively solving your own problems, I strongly suggest Anthony Weston's book, How to Re-imagine the World.
And here's a video advertising Poo Wi Fi. It's in Spanish, but never fear. You will NOT need to understand the language to fully follow what's going on. Enjoy!
 Clean Ones Pure Comfort reusable vinyl gloves are latex-free, BPA-free and phthalate-free. I'm not personally allergic to latex, a natural material from a rubber plant. But those who are can go into anaphlactic shock, so it seems like too big a risk to have them around.
Clean Ones Pure Comfort reusable vinyl gloves are latex-free, BPA-free and phthalate-free. I'm not personally allergic to latex, a natural material from a rubber plant. But those who are can go into anaphlactic shock, so it seems like too big a risk to have them around. Shipping small bottles is transportation-excess and creates too much CO2. I did find a 36 oz refill, and although the packaging is lighter weight than the bottles, it's not different enough size-wise to make the transportation-reduction impact a larger-sized refill - or even better, a concentrate product - could make. If someone knows whether Seventh Generation has a concentrate in this product, please let me know. I didn't see one on their website.
Shipping small bottles is transportation-excess and creates too much CO2. I did find a 36 oz refill, and although the packaging is lighter weight than the bottles, it's not different enough size-wise to make the transportation-reduction impact a larger-sized refill - or even better, a concentrate product - could make. If someone knows whether Seventh Generation has a concentrate in this product, please let me know. I didn't see one on their website.
 Clean Ones Pure Comfort reusable vinyl gloves are latex-free, BPA-free and phthalate-free. I'm not personally allergic to latex, a natural material from a rubber plant. But those who are can go into anaphlactic shock, so it seems like too big a risk to have them around.
Clean Ones Pure Comfort reusable vinyl gloves are latex-free, BPA-free and phthalate-free. I'm not personally allergic to latex, a natural material from a rubber plant. But those who are can go into anaphlactic shock, so it seems like too big a risk to have them around. Shipping small bottles is transportation-excess and creates too much CO2. I did find a 36 oz refill, and although the packaging is lighter weight than the bottles, it's not different enough size-wise to make the transportation-reduction impact a larger-sized refill - or even better, a concentrate product - could make. If someone knows whether Seventh Generation has a concentrate in this product, please let me know. I didn't see one on their website.
Shipping small bottles is transportation-excess and creates too much CO2. I did find a 36 oz refill, and although the packaging is lighter weight than the bottles, it's not different enough size-wise to make the transportation-reduction impact a larger-sized refill - or even better, a concentrate product - could make. If someone knows whether Seventh Generation has a concentrate in this product, please let me know. I didn't see one on their website.